As fall sports ramp back up, now is a good time to discuss ACL injuries.
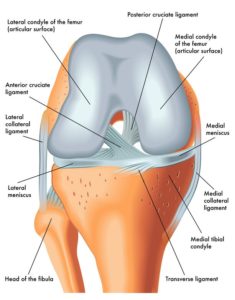
A.C.L. stands for Anterior Cruciate Ligament. The ACL is a strong ligament in the middle of the knee that plays an important role in knee stability. The ACL prevents the tibia from gliding too far forward and rotating in. We most often see ACL injuries when an athlete attempts to quickly change directions. Typically they will feel a pop in the knee and have immediate pain and difficulty bearing weight. Some athletes will start to feel better after a week or two when the swelling starts to subside. Some, even try to return to sport, not knowing the extent of their injury. Unfortunately, they tend to quickly find out that it is nearly impossible to return to competitive sports with a torn ACL as the knee will continue to be unstable with any pivoting movements.
In experienced hands, an ACL tear can usually be diagnosed by physical exam alone. However, it is standard to obtain an MRI to confirm the diagnosis and to check for additional knee injuries. Almost half will have some other knee injury (i.e. meniscus, MCL).
Once the diagnosis is confirmed, you should discuss your treatment options with an orthopedic surgeon who is experienced with ACL injuries.
Points to consider when discussing with your orthopedic surgeon should include: Timing of surgery, repair versus reconstruction, ALLOgraft versus AUTOgraft, graft type, treatment of any other present injuries, expected recovery, and long term function.
ACL repair vs reconstruction: ACL repair simply means the ACL tissue is left in place and reattached to its bony attachment site. Reconstruction means that the torn ACL tissue is removed and replaced with some other source of tissue.
ACL repair is only a feasible option if the ACL has pulled directly off its bony attachment on the femur (“avulsion”). This is only the case about 10% of the time. ACL repair is desirable because it is generally a less involved operation with a quicker recovery and return to sports. However, it also comes with the drawback of higher risk of retearing the ACL afterwards.
ACL reconstruction is a reliable operation that can get most athletes back to their competitive sports. ACL reconstruction can be broken down into 2 camps: 1. allograft and 2. autograft. Allograft uses donor tissue, from a cadaver. The grafts have been tested and are free of any sort of diseases or live cells. The donor tissue will eventually be “ligamentized” meaning that your own ligament cells will take over the graft, eventually turning it into your own living ligament tissue. Allograft comes with the benefit of a quicker surgery and less harm to your own tissue, because no tissue is being taken to use as your graft. However, this comes with a very big drawback, especially in the young athletic population, which is a much higher risk of retear!
Autograft means your own tissue will be used to make a new ACL.
There are 3 popular graft options that can be used to make your new ACL:
1. “BTB” Bone-patellar tendon-bone. 2. Quadriceps tendon and 3. Hamstring tendon. Each option comes with its own benefits and drawbacks but they have all been shown to be excellent options.
Finally, any additional injuries will need to be addressed at the time of the ACL surgery. Meniscus injuries are very common with athletic ACL injuries and should be treated with repair whenever possible. If a meniscus repair is necessary it will often necessitate delaying weightbearing after surgery for about 4 weeks.
Dr. Beard is a fellowship-trained sports medicine orthopedic surgeon with experience with each of these ACL treatment options. When treating the athletic ACL injury, there is a lot to consider and Dr. Beard will be able to answer all of your questions and guide you throughout the process. Please call to schedule a consultation if you would like to further discuss your treatment options.
(573) 756-7779.